 Book Appointment
Book Appointment
 +91 77740 40002
+91 77740 40002
×
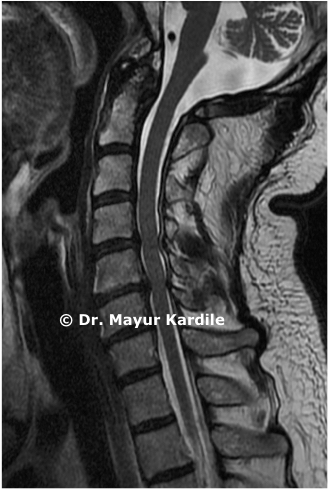
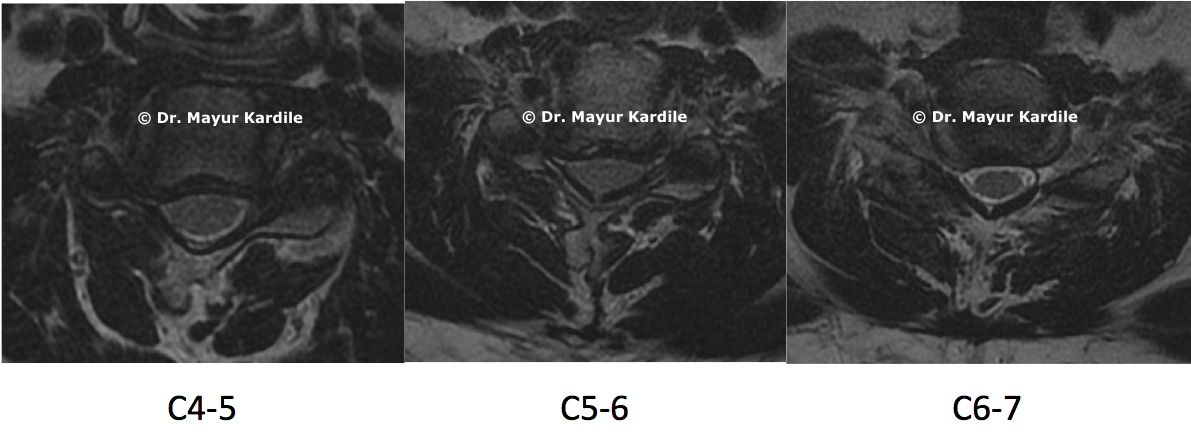
Patients with symptomatic, progressive cervical spinal stenosis and myelopathy undergo Anterior Cervical Corpectomy and Fusion (ACCF).
In Anterior Cervical Discectomy procedure the herniated disc in the cervical spine is removed and is replaced by a cage and bone graft to achieve fusion in the involved spinal segments.
Anterior Cervical Discectomy is performed to remove the large, arthritic osteophytes (bone spurs) that are compressing the spinal cord and spinal nerves. Almost the entire vertebral body and disc is removed and replaced with a piece of bone graft and fused together to maintain stability.
Cervical Disc Herniation, Ossified Posterior Longitudinal Ligament (OPLL), Infections and Tumors. ACDF anterior cervical discectomy and fusion. patients can get quick relief from neck and arm pain with this surgery.
The Anterior Cervical Discectomy surgery is performed under general anesthesia. Surgery is done through a small incision on the front part of the neck and patients can be discharged from the hospital in a day or two.
An endotracheal tube that is a breathing tube is placed and the patient breathes using a ventilator during the Anterior Cervical Discectomy surgery. Preoperative intravenous antibiotics are given to the patient. Patient is positioned in the supine position lying on the back, usually on a flat operating table. The surgical region of neck area is cleansed
A 2 to 4 cm transverse incision is made in one of the creases of neck, near the midline, depending on the number of levels. The cervical fascia is gently divided in a natural plane, between the esophagus and carotid sheath in the area containing the blood vessels in the neck. Retractors and an operating microscope are inserted to allow the surgeon to visualize the anterior that is front part of vertebral body and discs. After the retractor is in position, an x-ray is used to confirm that the appropriate spinal level is achieved.

When the compressive lesions are removed, the spinal cord and nerves may return to their usual size and shape with a full corpectomy and discectomy (removal of the cervical vertebral body and disc, including protruding osteophytes and disc fragments). Small dental-type instruments and biting/grasping instruments such as a pituitary rongeur and kerrison rongeur are used to remove the arthritic, hypertrophic that is overgrown bone spurs, including any spurs or disc fragments in the surrounding area. The size of the empty disc space is replaced with a right sized graft to restore the normal disc space height and the graft is then gently tapped into the space between the two vertebral bodies known as the disc. A small titanium metal plate is fixed to the vertebrae with small screws, to impart immediate stability to the construct and allow for optimal bone healing and fusion. The surgical wound area is closed using special surgical glue, leaving a minimal scar and requiring no bandage. The procedure requires about 2 hours depending on the number of spinal levels involved.
After the surgery physical therapists and occupational therapists train the patient on proper techniques of getting in and out of bed and walking independently. Discharge from hospital is given in 4 to 5 days after the surgery. Patient is trained for precautions to avoid bending and twisting of the neck, and heavy lifting for 4 to 6 weeks. Patient can gradually do that after 6 to 7 weeks as the pain decreases and the neck and back muscles get strength.